The London Centre for Male Chronic Pelvic Pain
If you are reading this web page, you have probably had chronic pelvic pain for a long time. You might have consulted several doctors, urologists and andrologists and have tried various different drugs, but despite these, your pelvic pain is still present and might return periodically.
Pain in the testicles, in the perineum, and suprapubic area makes it difficult to urinate, and sometimes pain can also be experienced during ejaculation, with a substantial impact on quality of life.
Do your symptoms seem to subside when you are relaxed in a warm place?
If so, you might have been wrongly diagnosed — rather than a prostate problem, you might instead have a disorder of the pelvic muscles, in the same way that calf cramp can arise when running. The London Centre for Male Chronic Pelvic Pain is devoted to researching and treating pelvic pain syndromes in men using the Castiglione–De Oliviera Protocol.
Pelvic pain syndromes treated in our centre include prostatitis, pelvic floor dysfunction, elevator ani syndrome, chronic pelvic pain syndrome (CPPS), and chronic abacterial prostatitis, among other diagnoses.
Our protocol was developed by Dr Fabio Castiglione and the physiotherapist André de Oliveira, director of the Alo Physiotherapy clinic in central London.
Dr Fabio Castiglione
History of the Castiglione – De Oliviera Protocol for Male Pelvic Pain

Dr André de Oliveira
It began with Andre De Oliviera, a Physiotherapist who had himself suffered from CPPS for many years. He contacted several urologists, including Dr Fabio Castiglione.
After taking a medical history and conducting a thorough examination of the pelvic muscles, Dr Castiglione explained to De Oliviera that the pain he felt was partly caused by pathological contractions of the pelvic muscles and that his prostate was fine.
They then began a programme of therapy based on shockwave therapy, muscle relaxant drugs, and prostate massage.
THROUGH MANY YEARS OF SUFFERING, Andre De Oliviera DISCOVERED A WAY TO BECOME FREE OF his pelvic pain.
De Oliviera was impressed by the benefits of the therapy and began to study physiotherapy techniques for relaxing the pelvic muscles. This growing interest has led him to attend international courses on the subject and travel worldwide to learn modern techniques to treat pelvic muscle pain.
In 2019 De Oliviera and Castiglione began to work together to treat men with diagnoses including chronic pelvic pain, prostatitis, elevator ani syndrome, pelvic floor dysfunction, myalgia, and other chronic pelvic pain syndromes. They have developed and implemented a new therapeutic protocol for male pelvic pain, combining the medical treatments and physiotherapy.
Their Protocol is based on the use of shockwave, muscle relaxant drugs, PDE5i and pelvic floor physiotherapy, incorporating advanced physiotherapy techniques. The intensity of the protocol is based on the characteristics of the patient.
The pelvis
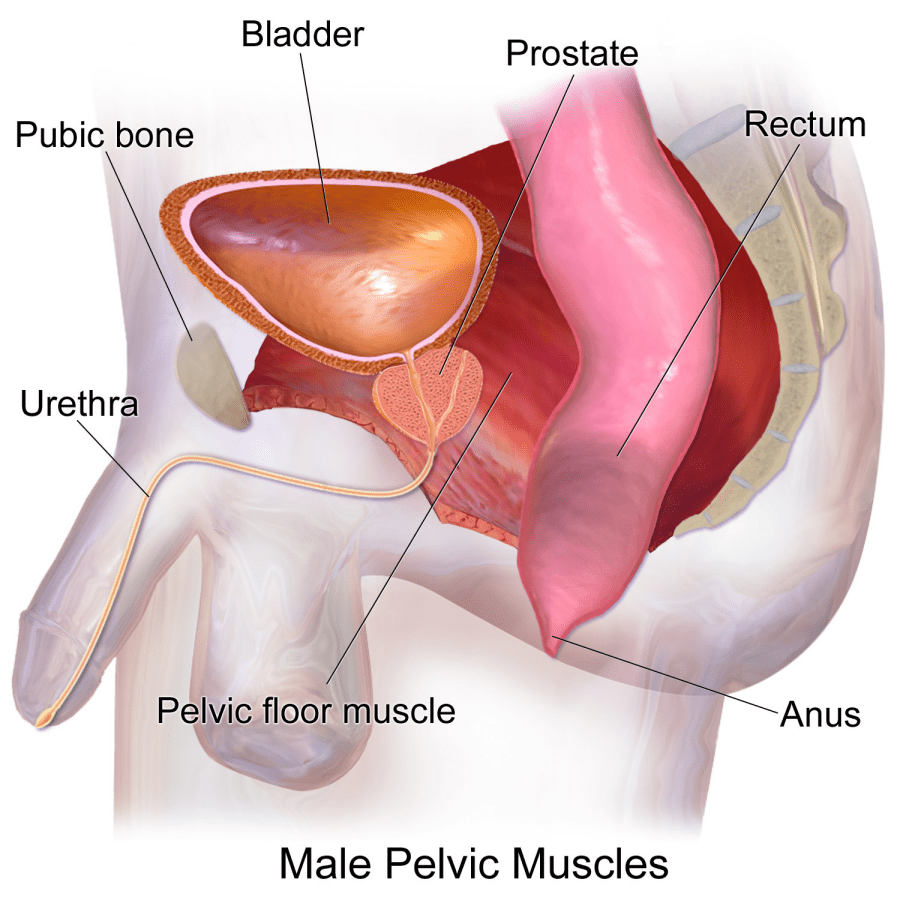
The pelvis is the anatomical region located below the navel, between the abdomen and the lower limbs. It is composed of the bones of the pelvis (ischium, pubis, iliac bones, sacrum and coccyx) that delimit the pelvic cavity, which houses various organs, muscles, nerves, blood vessels, and joints.
The organs contained in the male pelvic cavity are the kidneys, bladder, urethra, distal portions of the colon, prostate, seminal vesicles and vas deferens. The base of the pelvic cavity is called the pelvic floor, and the anatomical space below it — the perianal area between the testicles and the anus — is the perineum. Three holes cross the pelvic floor: the anterior one allows the passage of the vessels of the penis, the middle one through which the urethra passes, and a posterior one for the course of the rectum canal.
Given the anatomical and functional complexity of the pelvis, it is unsurprising that pelvic pain is common.
Unfortunately, pelvic pain is difficult to analyse as it is characterized by different symptoms attributable to pain or discomfort that can occur with varying intensity and in other areas. In general, patients mainly report localized pain in the lower abdomen, penis, testicles and perineum, with possible radiation to the lower back, groin, lower abdomen, and coccyx, as well as the upper thighs.
Intensity of the pain can vary from intermittent or continuous discomfort up to extreme, sometimes unbearable pain, sometimes described by the patient as stabbing pangs that interfere with activities of daily life.
The symptoms can be amplified during bladder emptying and filling, defaecation, erection, and ejaculation. Some patients notice that their pain disappears after defaecation, but typically this respite is for only a short period before the pain recurs. In some cases, the painful symptoms can increase if specific postures, such as sitting, are maintained for long periods.
Pelvic pain can be attributed to various causes, depending on the organ and/or structure affected. These include intestinal infections, inflammatory bowel diseases (for example, Crohn's disease), diverticulitis, appendicitis, constipation, inguinal hernia, haemorrhoids, urinary infections, urethritis, prostatitis, trauma and cancers affecting the intestinal, urinary or reproductive tracts.
Chronic pelvic pain (CPPS)
When a specific cause or underlying diagnosis cannot be identified, a diagnosis of chronic pelvic pain (CPPS) is made. CPPS is a common clinical syndrome with unknown aetiology and is often associated with urinary disorders and intestinal or sexual dysfunction.
In 1995, the US National Institute of Health (NIH) reclassified prostatitis into a more broad category of patients consisting of men who had the symptomatology of prostatitis but without inflammation and/or infection of the gland. This condition was designated chronic pelvic pain syndrome (CPPS) and is also known as chronic abacterial and non-inflammatory prostatitis type IIIB. This categorisation illustrates that the pathology of the condition cannot be attributed solely to prostate problems.
CPPS is a complex clinical situation characterized by a constellation of symptoms, alongside microbiological negativity of urine and semen and the absence of white blood cells in the prostate secretion. In addition, a high percentage of men who have CPPS have had non-bacterial prostatitis in the past.
Incidence of CPPS is increasing owing to improved methods of detection and its prevalence in a wide age-group of men from adolescence into old age. However, although it is often diagnosed, the causes of this syndrome are difficult to detect and are mostly unexplained.

- Genitourinary: urethritis, prostatitis, renal colic, inguinal hernia, prostate or bladder cancer, gonorrhoea and syphilis.
- Gastrointestinal: infections, inflammation and intestinal tumours.
- Neurological: anxiety, depression and excessive stress.
- Musculoskeletal: acute muscle stretching or inguinal and perianal lacerations, public and postural alterations.
Although these causes are known, the actual pathophysiology of CPPS is not well understood. However, involuntary hypertonia of the pelvic floor muscles (a pathological increase in muscle tone) is thought to underlie the syptomatology. In other words, chronic male pelvic pain is characterized by cramping or chronic spasm of the pelvic floor muscles.
Muscle cramping involves ischaemia — a reduced supply of oxygen to muscle cells, which activates anaerobic metabolism. As a result of anaerobic metabolism, toxic catabolites accumulate, the intracellular pH increases becoming acidic and vasoactive substances are released. These processes irritate the nerve endings present in the site affected by the muscle cramp, giving rise to a small inflammatory nucleus (trigger point) that is responsible for triggering the pain.
Fertility and quality of life

Shockwave therapy for CPPS
CPPS can be a disabling disorder with a substantial impact on the patient's fertility and quality of life. The pelvic floor musculature plays an essential role in sexual activity, as muscle contraction pumps blood into the penis, increasing intracavernous pressure and maintaining erection. In addition, the rhythmic contractions of the pelvic floor muscles contribute to propulsion of seminal fluid and, therefore, its subsequent emission.
Patients with pelvic pain can have difficulty maintaining an erection and/or achieving total stiffness. These sexual symptoms can lead to difficulties with intimacy and, consequently, to difficulties with conceiving, as they can result in avoidance of sexual intercourse.
In addition, chronic pelvic pain is almost always also associated with urinary and/or intestinal disorders that have repercussions on the patient's quality of life and can lead to anxiety and depression. Thus, careful diagnosis and treatment of this condition is important to address the symptoms and improve the patient's life.
Thus, when CPPS is diagnosed, the therapeutic options span several fields: pharmacology, psychology, shockwave, thermotherapy and physiotherapy.
The Castiglione – De Oliviera Protocol for Male Pelvic Pain has three phases:
The first phase consists of correctly diagnosing the condition. Dr Castiglione will perform a medical examination to identify the possible cause of pelvic pain:
- Genitourinary: urethritis, prostatitis, renal colic, inguinal hernia, prostate or bladder cancer, gonorrhoea and syphilis.
- Gastrointestinal: infections, inflammations and intestinal tumours.
- Neurological: anxiety, depression and excessive stress.
- Musculoskeletal: acute muscle stretching or inguinal and perianal lacerations, public and postural alterations.
If CPPS is diagnosed, medical therapy and shockwave treatment will be immediately started. This is known as the AMAPAS protocol:
- Alpha-blockers (which relax the prostate muscle and help passing urine)
- Myorelaxant drugs,
- Anticholinergic drugs (which relax the bladder muscle and help passing urine)
- PDE5 inhibitors (such as Viagra, which, when taken regularly can alleviate exercise-induced skeletal muscle ischaemia and improve muscle relaxation)
- Anti-inflammatories (including steroidal and non-steroidal anti-inflammatories as well as food supplements.
- Shockwave treatment, using low-intensity extracorporeal shock wave therapy (LI-ESWT), which has been reported to improve pain, urinary symptoms, and even sexual function by inducing neovascularization and anti-inflammation, reducing muscle tone, and influencing nerve impulses. In our Protocol, we usually perform
- 6–12 sessions based on the intensity of the pain.
Physiotherapy is critical for the multidisciplinary treatment of pelvic pain. Most patients suffering from chronic pelvic pain have hypertonia of the pelvic floor muscles and the abdominal muscles, which can be the primary cause of pain.
Our protocol uses several rehabilitation techniques: therapeutic exercise, vibration therapy and thermo-therapy. Through these conservative rehabilitation techniques, Mr Oliviera aims to reduce pelvic and abdominal muscle tension and, therefore, the resolve hypertonia. This approach seeks to break the vicious circle of ‘hypertonia–pain’ using individualized therapeutic pathways, to make the patient an active and conscious participant in their recovery.
Each of these treatments helps relieve pelvic pain symptoms, but none of them are able to eliminate the painful symptoms when used individually. Thus, a combination of pharmacological, physiotherapeutic, psychological, and behavioural therapies is required for proper rehabilitation of the pelvic floor, following each step of our protocol.