Benign prostatic hyperplasia
"Benign prostatic hyperplasia" Benign prostatic hypertrophy or hyperplasia is a pathology characterised by prostate gland enlargement.
The increase in prostate volume is linked to the rise in the number of epithelial and stromal prostate cells and the formation of nodules.
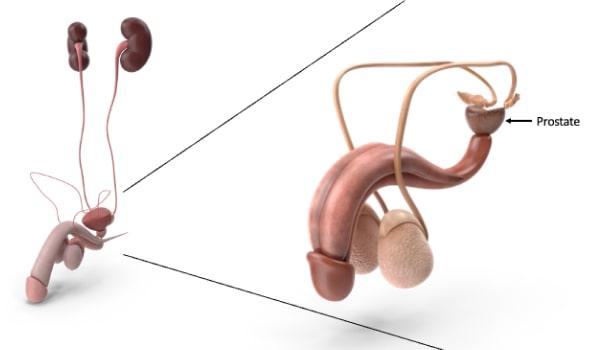
The enlarged gland can compress the urethral canal, causing a partial obstruction and interfering with the ability to urinate.
What is benign prostatic hyperplasia?
Benign prostatic hypertrophy or hyperplasia, also known as prostate adenoma, coincides with an increase in prostate gland volume, often due to ageing. This benign growth occurs in the transition zone of the prostate, compressing the prostate urethra and hindering urine leakage.
It is a widespread pathology in men; it affects 5–10% of men after 40 years of age and over 80% after 70 and 80 but produces symptoms only in half of the subjects. Such enlargement should not raise the excessive alarm because it is a benign and reversible pathology with no tumour formations and tissue infiltration.
Although the pathologies can coexist, scientific studies have not established any correlation between prostatic hyperplasia and carcinoma.
The main factors associated with the disease are ageing and hormonal changes in adulthood. Scientific studies have shown the existence of a genetic predisposition and familiarity. What are the symptoms of benign prostatic hyperplasia? Enlargement of the prostate gland leads to obstructive urinary symptoms and irritative ones. Compression on the urethral canal complicates urination. It is difficult to start urination due to intermittent flow emission, incomplete emptying of the bladder, weak urinary flow, and effort in urination. Irritative symptoms are frequency in urinating (pollakiuria), nocturia, i.e., an increased need at night, emptying the bladder (urgency) and burning while urinating.
How is benign prostatic hyperplasia prevented?
The best way to avoid benign prostatic hyperplasia is to get an early diagnosis by getting regular checkups after age 40–50 and acting quickly when problems arise. It is essential to follow a varied and balanced diet rich in fruits, vegetables, and whole grains but low in saturated fats (red meat, cheeses, and fried foods), avoiding chilli, beer, sausages, spices, pepper, spirits, coffee, and shellfish. It is essential to drink enough – at least two litres of water a day – and perform moderate and regular physical activity.
A urological examination with digital rectal exploration is often sufficient for diagnosing benign prostatic hyperplasia. The doctor can provide other tests practical to monitor the urinary flow and ascertain a possible failure to empty the bladder (uroflowmetry with an evaluation of the post-urination residue), establish the exact prostate volume if a non-destructive intervention is necessary (trans-rectal prostate ultrasound), and identify the dosage of PSA (prostate-specific antigen) by laboratory examination performed on a standard blood sample.

Specific drugs allow for the alleviation of urinary disorders associated with benign prostatic hyperplasia. However, among the side effects of their use, retrograde ejaculation (a phenomenon for which sperm is not ejaculated outside but introduced into the bladder) and excessive blood pressure reduction (orthostatic hypotension) decrease sexual desire.
TURP.
If the enlargement of the prostate is such as to provokes urinary obstruction, drug therapy is insufficient, and open surgery is required. Less invasive endoscopic techniques have supplanted traditional surgery: access to the prostate occurs transurethrally. We proceed to the resection of the central part of the gland (adenoma), responsible for the obstruction and the associated symptomatology.
The next step, starting in the nineties, was the introduction of a new endoscopic technique by laser, including the Holmium one. This treatment, minimally invasive, non-painful, and well tolerated by the patient, is called HOLEP (Holmium Laser Excision of the Prostate). After spinal anaesthesia, an instrument containing optical fibre and Holmium laser fibre is traced through the urethra to the prostate. With the laser fibre, we proceed to the enucleation of the adenoma, which is reduced into fragments (morcellation) and pushed outwards through the same instrument.
There are numerous advantages to this method, including the ability to intervene even on very voluminous prostates (for which the only alternative in the absence of lasers would be traditional open surgery); the removal of the bladder catheter only 24 hours after surgery; and a significant reduction in blood loss (post-operative blood transfusions are no longer required).Finally, the Holmium laser always makes it possible to perform a histological examination of the removed material, so it is possible to promptly recognise the presence of prostate tumours. The patient experiences an almost immediate improvement in urination, while burning and traces of blood in the urine tend to disappear within four weeks of surgery.
Rezum is an innovative treatment to treat benign prostatic hypertrophy developed in the United States and arrived in Europe in 2017-2018; it was born as an alternative therapy to surgical intervention to remove obstructive prostatic hypertrophy. Water vapour therapy is a minimally invasive procedure using natural energy stored in a few drops of water. It is possible to eliminate the excess prostate tissue that causes urinary symptoms.
How the intervention works The water vapour is injected with a very thin needle inside the hypertrophic prostate tissue (prostate adenoma), resulting in a progressive reduction in the prostate gland volume. This involves the normal resumption of urinary function and does not change the morphology of the apparatus, preserving all its functions.
The Advantages of the Rezum Technique There is no surgical scar.The intervention lasts about 15 minutes. The operation is performed in a day hospital or outpatient setting. In 85% of patients, general anaesthesia is not required to preserve ejaculatory function perfectly.
THE RESULTS
The results are obtained 2-3 months after treatment, allowing complete drug discontinuation. There is a marked improvement in urinary difficulties in a few weeks until the complete remission of the symptoms. The results are exceptionally long-lasting: on average, only 4% of patients must undergo surgery again within four years.The minimal invasiveness, the possibility of performing the procedure in a day hospital, the rapid resumption of daily activities, and the certainty of preserving ejaculation mean that Rezum is, to date, the cutting-edge technology for the treatment and definitive resolution of prostatic hypertrophy.