Male chronic pelvic pain
The pelvic floor is a cup whose walls are formed by a complex skeletal structure: bones, different muscles and ligaments. The various structures that make up the pelvic floor are not merely inert structures that delimit and close the lower wall of the abdomen.
The muscles that make up the pelvic floor contract, release, synergise, antagonise, and stabilise in coordination with the state of or activity of the pelvic organs. However, their function is not solely the control of visceral functions (urination, defecation, and coitus). The pelvic musculature also performs the critical task of supporting the organs in the abdominal cavity, maintaining their position, and assuming correct posture and walking.
Activity of skeletal muscles
Commonly the activity of skeletal muscles involves the displacement of one or more skeletal bones or segments caused by the combined action of agonist, antagonist, and stabiliser muscles. For example, flexing of the forearm, whereby the contraction of the brachial biceps pulls the forearm towards the upper arm and at the same time the antagonist muscle, the brachial triceps, is relaxed, and the shoulder muscles are stabilised.
However, this process does not happen with the pelvic floor muscles as, except for the visceral bundle of the puborectalis muscle, the pelvic floor muscles are mostly inserted into bone segments of the pelvis (the pubic, iliac, and sciatic bone), which are immobile. Therefore, their contraction does not cause bony movement. Instead the pelvic muscles' activity maintains a constant tonic situation (isometric contraction), which varies and increases only in certain circumstances, such as urination, defecation, and coitus. The tone of these muscles is unusual as it is constant and prolonged; thus, the pelvic muscles can be subject to exhaustion (which is typical of other muscle contraction) if a series of sophisticated neurological interactions at a non-cerebral level is avoided.
Chronic abacterial and non-inflammatory type IIIB prostatitis
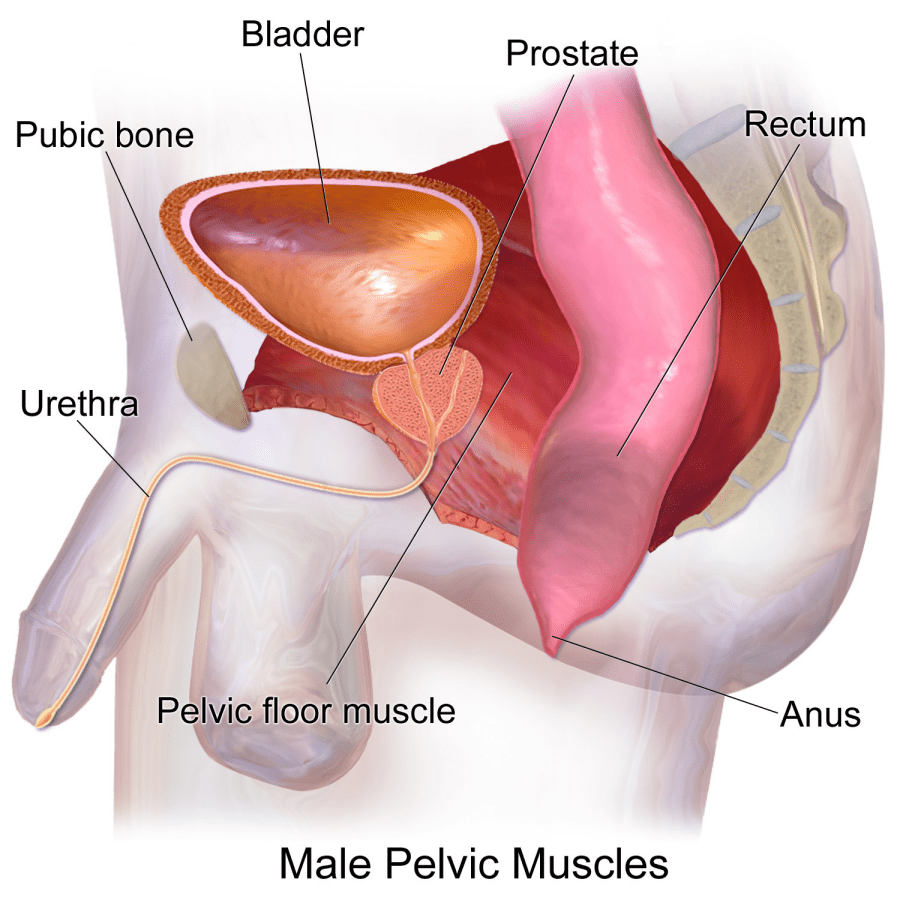
The prostate is a chestnut-sized male sex gland weighing ~20g located under the bladder, in front of the rectum, behind the pubic symphysis and above the pelvic floor.
Given the anatomical and functional complexity of the pelvic floor and its relationship with the prostate gland, pathologies of the pelvic floor and the prostate gland (prostatitis and chronic pelvic pain) can manifest themselves with pain in the lower abdomen, sometimes radiating to the testicles and penis, as well as urological, genital, and intestinal dysfunctions. The incidence of CPPS is on the rise because it is now more readily diagnosed and affects a broad age group of men, from 18 to 75 years.
In 1995 the National Institute of Health (NIH) reclassified prostatitis into four categories, owing to the fact that men with symptoms of prostatitis but without infection and inflammation of the gland comprised the most significant category. Thus, the cause of their symptoms could not reasonably be attributed to prostate gland problems alone.
This condition was referred to as 'chronic abacterial and non-inflammatory type IIIB prostatitis’ or ‘chronic pelvic pain syndrome', and is known by acronym of CP / CPPS.
CPPS is a complex clinical condition characterised by a constellation of symptoms, but negative microbiological tests of urine and seminal fluid (known as a negative Meares-Stamey test) and the absence of white blood cells in the prostate secretion. In CPPS, the patient reports pain that can be localised in the pelvic region, in the perineum (the space between the testicles and the anus) with possible radiation of the pain to the lumbar region, to the external genitalia (testicles and penis), the groin, the suprapubic area (towards the belly button), the sacrococcygeal region (the lower back just above the buttocks), or the root of the thighs.
These painful symptoms are sometimes accompanied by difficulties with voiding, colon or proctological symptoms and sexual symptoms such as erectile dysfunction, decreased desire, premature or delayed and sometimes painful ejaculation.
Ache
CPSS can involve many different types of. First, the intensity of the pain is variable, ranging from a vague sense of continuous discomfort up to extreme, sometimes intolerable pain, the some patients describe as ‘excruciating’.
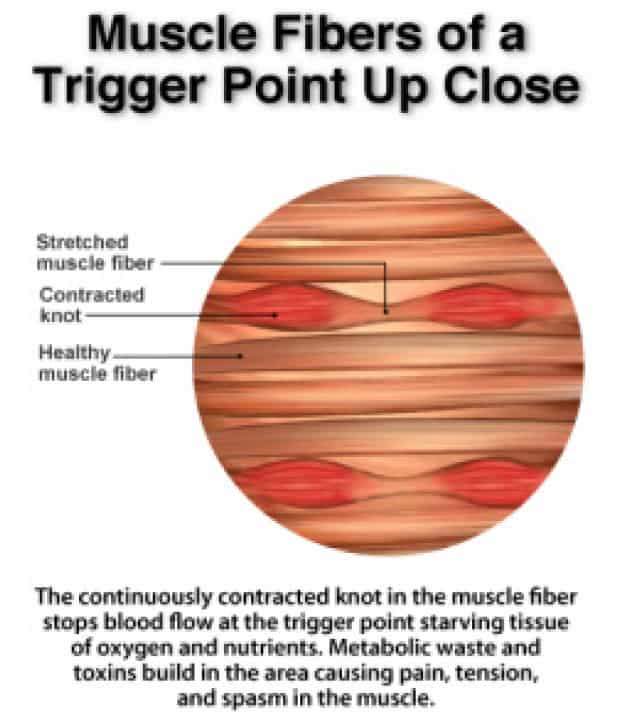
In some cases, the painful sensation seems to be related to the filling or emptying of the bladder and rectum, whereas in other cases, it is caused by particular positions, such as sitting, or by the pressure exerted on specific points in the pelvic area, called trigger points. Unrecognised persistent pain without a definitive diagnosis can lead to stress, irritability, and depression.

Various voiding symptoms may coexist in CPPS throughout the different phases of bladder filling and emptying.
In the pre-voiding phase, which is sustained by hypertonicity or by a failure to relax the external urethral sphincter, pain can cause inhibition of the urination reflex, and the symptoms are then characterised by hesitation of urination, abdominal press required for urination, and urinary retention.
During the bladder filling phase, muscle hypertonicity will result in frequent urination stimulus both during the day (pollakiuria) and at night (nocturia) which is rarely associated with a picture of detrusor hyperactivity on urodynamic studies.
In the voiding phase, muscle hypertonicity hinders urinary flow resulting in an unreliable, intermittent urine stream, a sensation of incomplete emptying and residual urine remaining in the bladder after voiding. The variable presence of a post-voiding residual can cause recurrent urinary infections which can be associated with sudden worsening of the frequency of urination and the onset of burning and pain with urination.
The pelvic floor musculature plays a vital role in sexual activity: the contraction of the ischium and bulbocavernous muscles force the blood into the penis by increasing intracavernous pressure, while contractions of the Houston's muscles reduce the venous discharge of the erect penis, helping to maintain a full erection. Finally, the rhythmic contractions of the bulbocavernous muscle cause the propulsion of the seminal fluid and, therefore, its emission. Thus, pelvic floor dysfunction could play a role in the genesis of some sexual dysfunctions. In chronic prostatitis, sexual symptoms can affect all phases of the sexual response: desire, arousal, and orgasm.
Notably, studies have highlighted difficulties in maintaining an erection in young men with prostatitis. This difficulty in maintaining an erection or achieving complete rigidity is known as a veno-occlusive syndrome; during CPPS, it is caused by damage to the venous valves of the penis by chemicals produced by the inflammatory process in the prostate.
Effects on quality of life

Chronic pelvic pain can be a debilitating disorder with a considerable impact on the individual's quality of life. Clinical studies have shown that chronic discomfort in the pelvis, generated by a prolonged condition of discomfort or pain, can translate into anxiety, depression, and alteration of self-image and self-esteem. Furthermore, stress can amplify feelings of discomfort perceived in the lower abdomen.
Thus, pain and anxiety create a vicious circle capable of profoundly altering the quality of life of the patient, limiting daily activities and social and relational activities. The couple's relationship might also be compromised, especially in the presence of sexual dysfunctions, resulting in reduced frequency of sexual intercourse or even avoidance.
Various different pathological conditions can cause chronic pelvic pain syndrome (CPPS):
- Relapsing prostatitis
- Perineal trauma
- Acute muscle strain
- Postural alterations
- Excessive gymnastic activity that increases the tone of the pelvic muscles with incorrect or absent stretching
- Excessive Stress and muscular and emotional tensions
The exact pathophysiology of CPPS is not yet fully known understood. However, it is believed to be determined by several factors, which ultimately result in a chronic neuropathic and muscle pain syndrome and the common pathophysiological alteration that induces the symptoms is an involuntary hypertonicity of the pelvic floor muscles.
Pain in CPPS is characterised by a chronic cramp or spasm of the pelvic floor musculature. Chronic muscle spasm leads to ischaemia (lack of oxygen) and, therefore, a reduced oxygen supply between the muscle fibre cells. This leads to anaerobic metabolism with a series of cascading sequelae, including creating of an acidic intercellular environment, accumulation of toxic waste substances (catabolites such as lactic acid or calcium ions), lymphocyte infiltration and the release of vasoactive substances such as colchicine, which irritate nerve endings.
Dr Andre De Oliviera and Dr Castiglione worked together for 3 years to develop and implement a new therapeutic protocol for male pelvic pain combining medical and physiotherapy treatments for CPPS, including prostatitis, levator ani syndrome, pelvic floor dysfunction, myalgia, and other chronic pelvic pain syndromes.
The protocol is based on the use of shockwave therapy, muscle relaxant medication, PDE5 inhibitors and advanced physiotherapy techniques to the pelvic floor. The intensity of the protocol is based on the characteristics of the patient.